This week, I will give you five nursing diagnosis for bronchitis.
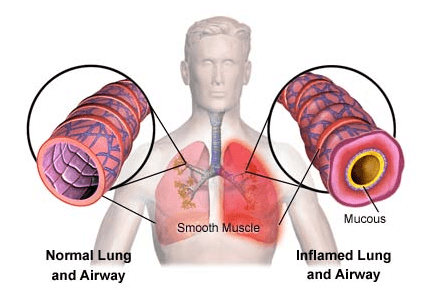
1) Ineffective airway clearance related to increased mucus production. Thick mucus production is a signature sign and symptom of bronchitis, especially chronic bronchitis. Our goal for patient would be to clear airway effectively with nursing intervention such as drinking 3 liters of water a day to thin out mucus.
2) Activity intolerance related to ineffective ventilation and oxygenation. Having constant shortness of breath and coughing while moving around are the major complaints from patients with bronchitis. This is significant because it means you can't take a shower, grocery shopping, walking down the street without catching your breath or having trouble breathing. Our nursing goal for the patient would be to tolerate daily activities without trouble breathing with nursing intervention such as daily activity such as short distance walking with time increment as tolerated. If patient is in the hospital, maybe he/she would walk around the unit once a day and distance and frequency would increase as the patient can tolerate.
3) Anxiety related to changes in health status. It is scary to have bronchitis because you can't breathe properly. It can be overwhelming to adjust to your new health condition. You can't live your life like you used to before you have bronchitis. If you have chronic obstructive pulmonary disease (COPD), you will not be cured from it. Treatment would only treat your symptoms which do not go away. Our nursing goal for patient would be able to cope with current medical condition with friends and family with nursing interventions such as education about the illness, education about local support group, etc.
4) Ineffective breathing pattern related to bronchoconstriction and excessive mucus. When you have bronchitis, your bronchi would constrict and thick mucus would be released. It can clog up your airway making you suffocate. Some patient with COPD with acute exacerbation would require suctioning and ventilation to breathe and to maintain a patent airway. Our goal would be to breath effectively by using pursed-lip breathing technique and sitting in a tripod (semi-fowler) position. It will be the nurse's responsibility to teach the patient these techniques and to practice with the patient.
5) Acute pain related to inflammation in pleura (the thin sheet mucous tissue that wraps around your lungs). You will hurt whenever you breathe. Our goal is have patient's pain manage at a comfortable level per patient's report.
|
Actual/Potential
|
related to
|
plan/outcome
|
nursing intervention
|
|
Actual pain
|
related to inflammation in pleura
|
manage pain/ patient will report 3/10 pain by the end of shift.
|
offer routine/prn pain medication accordingly, assess patient’s pain
level during hourly rounds.
|
Reference:
NCP NANDA. (n.d.). Retrieved February 26, 2015, from http://ncpnanda.blogspot.com/2013/02/9-nursing-diagnosis-for-bronchitis.html
(n.d.). Retrieved February 26, 2015, from http://faculty.mu.edu.sa/public/uploads/1380604673.6151NANDA 2012.pdf